
From the moment researchers began investigating the hypertrophic and strength adaptations achieved through blood flow restricted exercise, nearly every discussion section of every published paper included some version of, “It seems like this technique would be quite valuable to the rehab community.” Well, these musings are certainly being realized today in musculoskeletal rehab. And while researchers posed these curiosities, they carried on attempting to elucidate the overall safety of the technique as a number of questions were important to answer. Two questions were of paramount concern:
- Will BFR cause a clot?
- What are the hemodynamic implications?
We’ll tackle blood pressure and heart rate responses in another blog, and previously we’ve tackled the VTE question more broadly. For this blog we’d like to put out some thoughts on whether or not BFR exercise should be considered if your client has an inherited thrombophilia. If you recall from our podcast on VTE, Ben showed everyone up with his pronunciation of Virchow’s Triad (fact check: it’s actually pronounced “fear-hoff” not “fear-chow”), but also that Virchow’s Triad is important foundational knowledge for understanding the risk of VTE. That knowledge will help us reason through whether or not to use BFR on a person with an inherited thrombophilia. Here’s a graphic we made to illustrate Virchow’s Triad:
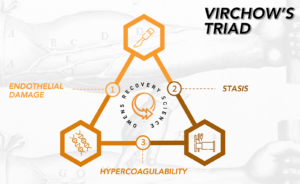
Inherited thrombophilias will fall under the hypercoagulability portion of Virchow’s Triad. An important point regarding hypercoagulability is that it encompasses both “acquired” and “hereditary” forms. “Acquired” hypercoagulability refers to a circumstance that happens to a person. The easiest way to think about that is surgery; you’ll get both endothelial damage from any incisions and stasis from reduced physical activity which will combine for increased acquired hypercoagulability. To better understand the inherited thrombophilias it is helpful to grasp the basic principle that at any point in time our body is cycling through the expression of coagulation or anti-coagulation factors. For illustration purposes, we could draw a parallel to how at any given point in the day the human body is either trying to make muscle via muscle protein synthesis or break it down via muscle protein breakdown. Persons with thrombophilia have elevated resting levels of coagulation factors or decreased levels of anti-coagulation factors. This, combined with endothelial damage or stasis further amplifies an already elevated level of clot formation risk since the body is not clearing these factors as easily due to stasis, or it is actively trying to clot in response to damage.
Our approach to reasoning through any safety concerns related to BFR is to first identify what the potential concern is, investigate any literature on that condition / injury / etc. to flesh out more specifically what to look for, and then to assess the surgical tourniquet and exercise literature for any evidence that they influence our concern positively or negatively. We then will cull the BFR literature for anything that has specifically looked at our concern.
Here’s a sample of how we might think through the use of BFR in the presence of an inherited thrombophilia:
- What is our concern? Our concern is that BFR might increase one’s risk of clot formation in persons with inherited thrombophilias.
- What do we know regarding why someone with an inherited thrombophilia forms a clot? From the Bond paper in JOSPT we know that it’s very uncommon for a person with a thrombophilia to spontaneously form a clot. Clot formation is almost always tied to an acquired form of hypercoagulability.
- What does the literature say re: use of surgical tourniquets on persons with inherited thrombophilias? Nothing
- What does the exercise literature say re: risks to persons with inherited thrombophilias? Nothing
- What does the BFR literature say re: risks to persons with inherited thrombophilias?Absolutely nothing
Well that clears things up nicely doesn’t it? Obviously not, but this circumstance is pretty common when trying to make a reasoned decision with BFR as it pertains to the current literature base. We’ve said time and again the literature is very limited on clinical applications, and those of you that have reached out with questions or posted in our Inside Circle know all too well that we routinely give you a ¯\_(ツ)_/¯ when posed a question related to an uncommon or at times common condition. We do, however, have a number of papers that have examined the use of BFR both acutely and chronically on factors that indicate endothelial damage or stasis. To date no study has pointed to BFR amplifying either of those. Combining that with the knowledge that thrombophilias have a low prevalence, Factor V Leiden is the most common at 3-7% of the US population, and clots are very rare in the absence of an acquired hypercoagulability, even in those with thrombophilia, gives us a framework from which to make a good clinically reasoned decision.
OUR GUIDANCE...
Shared decision making is the bedrock of any intervention that a healthcare provider delivers. If your patient in fact knows they have a thrombophilia and has no history of VTE, the odds are, based upon what we’ve presented you here that they will be just fine. But, you should discuss with them that there is no specific literature as it pertains to their thrombophilia and BFR exercise making it impossible to know one way or the other what the true risk is. If your patient has a history of VTE, or recently had surgery, this decision gets substantially more difficult as your client’s risk for clot is exponentially increased. In this circumstance there should definitely be some consultation with the referring MD and potentially your patient’s hematologist. It’s our opinion that the medical team, along with the patient, must all agree that BFR is a very important piece to a successful course of care and is worth the potential risk that a clot may occur given all the factors on board.
We hope this is helpful! Stay tuned for our upcoming blog on hemodynamic responses for Ben! We’ve provided some additional resources on VTE and thrombophilia below.
