
As more and more papers come out using a variety of parameters for blood flow restriction training or occlusion training interventions we are routinely asked if we have new protocols to share. From our perspective, any and all protocols have flaws, and oftentimes those flaws are rather large and unavoidable. Thus, we generally try to avoid them, opting instead to teach principles of exercise prescription and how to adjust those in relation to physical therapy or rehabilitation and the use of BFR. In reading a recent paper written to summarize the existing literature on blood flow restriction training with endurance exercise, a line from the paper prompted me to try and map out the many variables and criteria one should have a mastery of in order to manipulate a blood flow restricted exercise intervention in a comprehensive manner. Ferguson et al wrote, “In many respects, the permutations of intensity and duration of exercise and the application of BFR are endless.” (Ferguson et al., 2021)
Below is a list of most of the variables you can manipulate for a given exercise session:
PROBABLE BFR EXERCISE VARIABLES:
- Pressure: Percentage of Limb Occlusion Pressure (LOP = the minimum pressure needed to stop arterial blood flow in a limb)
- Pressure Application: Continuous or Intermittent
- Load
- Task
- Rep / set scheme
- Effort
- Load progression / regression
Any number of factors could play into why you might adjust the aforementioned variables with the use of BFR training. For example, perceptual responses like discomfort could be addressed via pressure reduction until tolerance increases. Another strategy to alleviate discomfort would be to deflate the cuff between sets two and three or incorporate some form of intermittent blood flow restriction. Difficulty completing the rep / set scheme with bfr training could be the result of the load being too heavy, or perhaps the task itself was just too complex or difficult. If the load was too heavy, try reducing the weight and see if that makes it easier to complete the reps / sets. If the task was just too difficult or complex, try breaking it down into smaller, more manageable pieces.
In today’s Instagram world, an oft perpetuated myth is that the more complex and “cool” an exercise is, the more effective it is. These “circus bear exercise feats” are often followed by some word salad explanation that is very confident, and in effect hypnotizes the reader into thinking the author must clearly know more than the reader regarding exercise prescription. Well, the good news is that exercise does not need to be complex in order to create changes in muscle size and strength. In fact, the more complex an exercise, the more varied the adaptations or lack thereof may be and this seems to hold true when resistance exercise is combined with a BFR cuff. A nice example of that can be found in the paper we reviewed on our most recent podcast. The authors described why they favored a single joint strength assessment over a multi-joint assessment as follows, “...and single joint > multiple joint strength test. This approach was chosen in order to minimize outcome variability by favouring low exercise neuromotor difficulty (e.g. knee extension > leg press).” (Grønfeldt et al., 2020) The more complex an exercise task, the more options there are for how to complete it. This has also been detailed very nicely in two papers from researchers at USC who showed that even to the trained eye, picking up on how someone alters their strategy to complete a task as simple as a squat is virtually impossible. (Chan & Sigward, 2019, 2020) Thus, in order to force a muscle to work hard enough to elicit a change even with low load resistance training and BFR, at minimum one must consider if there’s an escape for that muscle via an alteration in strategy, and control for it by constraining the movement.
Effective prescription of exercise with and without blood flow restriction requires that you have a goal for the exercises you choose. Presently, some targets for exercise with blood flow restriction that have an established evidence base are pain reduction, or increases in endurance, hypertrophy, or strength. Hughes et al have indicated that higher percentages of blood flow occlusion may play a role in the magnitude of hypoalgesia. (Hughes & Patterson, 2020) They've shown this with resistance exercise combined with BFR as well as low-intensity cycle training with restricted blood flow. (Hughes et al. 2021) Guidance for endurance, hypertrophy, and strength were nicely detailed in the 2019 methodology paper spear-headed by Stephen Patterson, PhD. (Patterson et al., 2019) Additional benefits of blood flow restriction training are of course possible, but at least one of these should comprise the reason for choosing BFR.
In addition to having a treatment and / or parameter target based on current evidence, inherent limitations in rehab will result in the clinician inevitably encountering scenarios where BFR may be used in a strategic fashion to progress toward more optimal parameters, or progress away from the intervention altogether. This is why we’d suggest having a performance as well as a progression target to help you determine when to modify the intervention. With that in mind, simple aerobic type tasks combined with blood flow restriction can serve as a bridge to more difficult resistance training with blood flow restriction as the patient gains ROM, and the ability to complete a high volume of work. Those early visits with low level activity can be used to familiarize w/ blood flow restriction pressure as well as with engaging fatigue at a lower intensity than will ultimately be necessary to build muscle. Early phase interventions like combining BFR w/ NMES can also contribute in this way, but could have a place later in rehab as a finisher too.
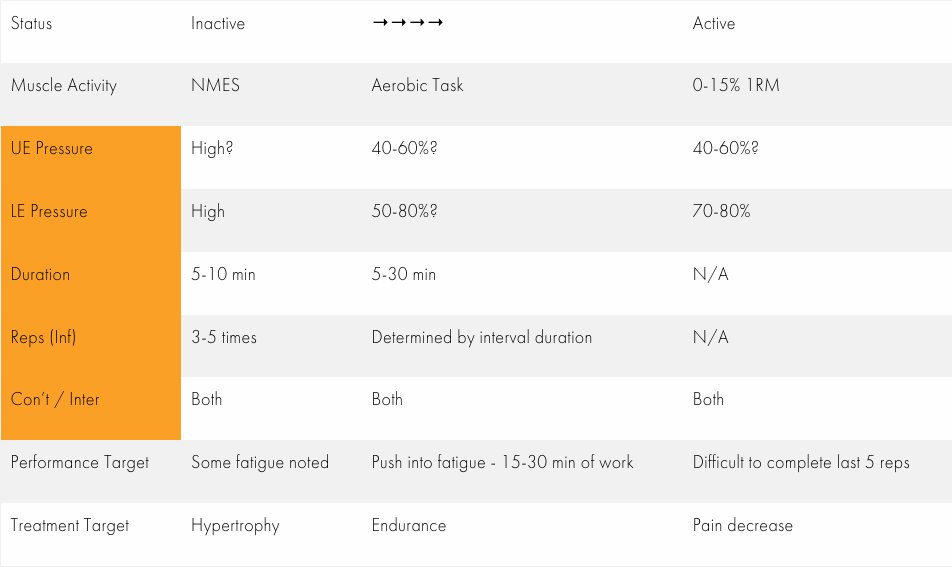
Some simple adjustments to variables can help the clinician gain buy-in from his or her patient, while exposing them gradually to an intervention. If you’re like me, you probably undershoot the load initially. This can work well as an introduction to BFR though. It does however require that you be mindful of effort and progress load as soon as possible. I watch rather intently how well my patient completes their last set of 15. Did I have to encourage them, did I have to assist them, or did they finish with just some minor effort? These are questions that help me determine how to adjust their next visit. If they make it through all 75 reps 2 visits in a row, load goes up. Sometimes it is obvious you have undershot and merely adding exercise volume to get more effort on the fly is certainly an option. Then make a note to progress the load the next visit. Other times a patient might really be having a tough time with the pressure. In those cases you can of course reduce the pressure, but you could also fully deflate during the rest period (to do this with a Delfi, disconnect the hose from the cuff and cover it with your thumb...pushing deflate will force a 1 minute rest). That’s just a sampling of how to think through your BFR exercise. Below you will also find a sample of a chart I made to help me think through the many variables I need to be attending to and modifying!
References:
- Chan, M.-S., & Sigward, S. M. (2020). Center of pressure predicts Intra-limb compensatory patterns that shift demands away from knee extensors during squatting. Journal of Biomechanics, 110008.
- Chan, M.-S., & Sigward, S. M. (2019). Loading Behaviors Do Not Match Loading Abilities Postanterior Cruciate Ligament Reconstruction. Medicine and Science in Sports and Exercise, 51(8), 1626–1634.
- Ferguson, R. A., Mitchell, E. A., Taylor, C. W., Bishop, D. J., & Christiansen, D. (2021). Blood-flow-restricted exercise: Strategies for enhancing muscle adaptation and performance in the endurance-trained athlete. Experimental Physiology. https://doi.org/10.1113/EP089280
- Grønfeldt, B. M., Lindberg Nielsen, J., Mieritz, R. M., Lund, H., & Aagaard, P. (2020). Effect of blood-flow restricted vs. heavy-load strength training on muscle strength: Systematic review and meta-analysis. Scandinavian Journal of Medicine & Science in Sports. https://doi.org/10.1111/sms.13632
- Hughes, L., & Patterson, S. D. (2020). The effect of blood flow restriction exercise on exercise-induced hypoalgesia and endogenous opioid and endocannabinoid mechanisms of pain modulation. Journal of Applied Physiology. https://doi.org/10.1152/japplphysiol.00768.2019
- Hughes, L., Grant, I., & Patterson, S. D. (2021). Aerobic exercise with blood flow restriction causes local and systemic hypoalgesia and increases circulating opioid and endocannabinoid levels. Journal of Applied Physiology. https://doi.org/10.1152/japplphysiol.00543.2021
- Patterson, S. D., Hughes, L., Warmington, S., Burr, J., Scott, B. R., Owens, J., Abe, T., Nielsen, J. L., Libardi, C. A., Laurentino, G., Neto, G. R., Brandner, C., Martin-Hernandez, J., & Loenneke, J. (2019). Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Frontiers in Physiology, 10, 533.
