
The measurement of Limb Occlusion Pressure (LOP) takes into account variables related to the tourniquet as well as variables specific to the individual. Individual variables such as limb circumference, tissue characteristics under the cuff, and systolic blood pressure all influence LOP. Blood pressure is influenced by body position, and of course rises when transitioning from supine to sitting or standing. The increase in blood pressure is a result of mechanical deformation of the vessel and stimulation of group III/IV afferents. This has led many to ask, “should LOP be assessed in the position the patient is exercising to more accurately determine LOP and subsequently the relative occlusion pressure used during the exercise?”
Recently, Sieljacks and colleagues looked at the difference in LOP between supine and sitting.(Sieljacks et al. 2018) When using a wide tourniquet, the authors found a 29 mmHg increase in LOP when measuring LOP in sitting compared to supine. Using this data in a subsequent knee extension study(Sieljacks et al. 2018), Sieljacks measured LOP in sitting, which was the position individuals were going to exercise. Although the authors measured LOP in sitting, they decided to use a relative occlusion pressure of 40% that produced a similar amount of occlusion as 50% LOP measured in supine, which was used in their previous projects.
Hughes et al expanded on this by comparing LOP measurements in supine, sitting and standing.(Hughes et al. 2018) When compared to supine, measuring LOP in sitting resulted in a 17 mmHg increase ; whereas in standing LOP was 54.5 mmHg higher. Applying this in a clinical context, Centner et al had individuals perform seated and standing heel raises using either high loads or low loads with BFR.(Centner et al. 2019) The BFR group performed each exercise with a relative pressure of 50% occlusion, which was assessed in standing. When measuring LOP in standing, a relative pressure of 50% occlusion roughly translates to a relative occlusion of 65% LOP measured in supine. This is important clinically because many times individuals are performing multiple exercises in different positions (sitting, lying, standing). If we set the relative pressure at 80% measured in standing, but also have them perform a supine exercise such as a SLR or leg press, the 80% LOP taken in standing will likely place that individual at full occlusion in supine. Conversely, if LOP is measured in supine, and the clinician then has a patient perform squats using a low pressure (60% LOP),the relative pressure would be much lower, approximately 45% LOP. A relative pressure this low has been shown to significantly limit the effectiveness of BFR, however, studies showing this low a pressure as ineffective were performed in a seated position rather than standing.
Collectively these papers suggest, if performing a single exercise, one can assess LOP in the position the exercise will be performed. However, an important limitation to the available evidence is the two referenced papers have only assessed an acute change in LOP. We do not know if there is a significant difference in muscle activation acutely, nor do we know how this impacts adaptation in the form of strength and hypertrophy. We would emphasize that when determining the appropriate pressure to use, we want to select the lowest pressure known to have an effect. Not only will using the lowest relative arterial occlusion pressure possible make the exercise more tolerable, but the lower pressure will also minimize the risk of an adverse event. To this end, if you plan to have your patient perform multiple exercises in varied positions, we would suggest a simple strategy that we teach in our courses of measuring in supine and following the guideline of using a 60-80% LOP. If performing a single exercise, you may perform LOP in the position of the exercise. To do that just follow the table below:
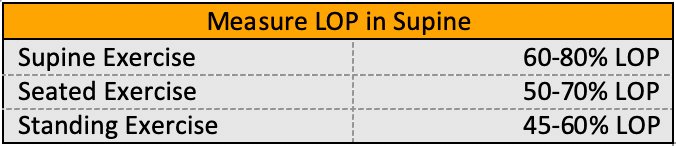
(for loads < / = 30% 1RM use highest pressure)
A big thanks to Zac Dunkle, PTfor this write up!!
- Sieljacks, P., Knudsen, L., Wernbom, M., & Vissing, K. (2018). Body position influences arterial occlusion pressure: implications for the standardization of pressure during blood flow restricted exercise. European Journal of Applied Physiology, 118(2), 303–312.
- Hughes, L., Jeffries, O., Waldron, M., Rosenblatt, B., Gissane, C., Paton, B., & Patterson, S. D. (2018). Influence and reliability of lower-limb arterial occlusion pressure at different body positions. PeerJ, 6, e4697.
- Centner, C., Lauber, B., Seynnes, O. R., Jerger, S., Sohnius, T., Gollhofer, A., & König, D. (2019). Low-load blood flow restriction training induces similar morphological and mechanical Achilles tendon adaptations compared to high-load resistance training. Journal of Applied Physiology. https://doi.org/10.1152/japplphysiol.00602.2019
